Introduction: Welcome to my blog! I am U.AKANKSHA a 4th year medical student.This is an online E-log Entry Blog to discuss, understand and review the clinical scenarios and data analysis of patients so as to develop my clinical competency in comprehending clinical cases, and providing evidence-based inputs.It also reflects patient centered online learning portfolio.
Note: The cases have been shared after taking consent from the patient/guardian. All names and other identifiers have been removed to secure and respect the privacy of the patient and the family.
Consent: An informed consent has been taken from the patient in the presence of the family attenders and other witnesses as well and the document has been conserved securely for future references.
A 60 year old female presented to Casuality with,
CHIEF COMPLAINTS:
Left Flank pain since 12 days
Fever since 10days
Burning micturition since 10days
Increased frequency of micturition since 10days
Vomitings since 2days
HISTORY OF PRESENTING ILLNESS:
Patient was apparently asymptomatic 12days ago, she then developed pain in Left flank since 12days.
-Insidious and gradually progressive, radiating
from left flank to groin
-Spasmodic and pricking type of pain
Fever since 10days
-High grade
-Associated with chills and rigors
-Relieved with medication
Burning micturition since 10days
Increased frequency of micturition since 10days
Vomitings since 2days
-Content food material
-Non bilious
-Non projectile
-Not blood stained
DAILY ROUTINE:
Patient is a Fruit seller by occupation.
She wakes up at 6am, has breakfast at 6:30am, goes to work at 10am, has lunch around 1-2pm, comes back home at 6 pm, has dinner at 9pm and goes to sleep around 10-11pm.
Since 10days she hasn't been able to go to work due to Left flank pain and body pains.
PAST HISTORY:
Patient is a known case of Diabetes Mellitus type 2 since 25years , on Tab. Glimi -M2 PO/OD
Patient is a known case of Hypertension since 25years, on Tab.Amlong 5mg PO/OD
History of Hysterectomy 23years ago
PERSONAL HISTORY:
Patient complains of body pains and decreased appetite since 10days
Bowel movements are normal
History of pruritis seasonal(summer)
FAMILY HISTORY:
No similar complaints in the family members.
GENERAL PHYSICAL EXAMINATION:

Examination has been done in a well lit room in supine and sitting position after taking informed consent and after reassuring the patient.
-Patient was conscious, coherent, cooperative and well oriented to time, place and person.
-Pallor present
No signs of Icterus , Cyanosis, Clubbing,Oedema, Lymphadenopathy, Malnutrition, Dehydration, Generalized lymphadenopathy
SYSTEMIC EXAMINATION:
Central Nervous System : No abnormality detected.
Per abdomen: Soft, Tenderness in Left Iliac fossa, Left lumbar region.
Cardiovascular system: S1, S2 heard, No murmurs
Respiratory system: BAE+, NVBS+
VITALS:
BP- 140/90 mm Hg
RR- 18 cpm
PR- 96 bpm
SpO2- 98%
Afebrile
INVESTIGATIONS:
Prorthrombin Time
APTT
Serum Electrolytes
Serum Creatinine - #1.3
Liver Function Test
Blood Urea
RBS - # 221
Serum Iron
Reticulocyte count
Hemogram
Blood Urea
BGT
Bleeding &Clotting time
Radiological investigations
PROVISIONAL DIAGNOSIS:
ACUTE PYELONEPHRITIS with TYPE 2 DIABETES MELLITUS & HYPERTENSION with ANAEMIA
TREATMENT:
1) IV Fluids NS at 80ml/hour
2) Injection Piptaz 2.25gm IV /TID
3) Injection Neomol 1gm IV/SOS
4) Injection Optineuron 1amp in NS at 50ml/hour
5) Check GRBS 7th profile
6) Injection HAI S/C TID
7) Injection NPH S/C BD
8) Tab. Cinod 10mg PO/BD
9) Injection Zofer 4mg IV/SOS
10) Injection Pan 40mg IV/OD
11) Injection Tramadol 1amp in 100ml NS IV/SOS
20/7/23
Abdominal pain decreased
No fever spikes, vomitings
O: patient is c/c/c
Temp: 98.5 F
PR: 74 bpm
Bp: 170/100 mmhg
RR: 18/min
Spo2 - 92% on RA
CVS: s1 s2 heard
No murmurs
Rs: BAE +
NVBS
CNS: NAD
P/A : soft
Tenderness + in left flank and suprapubic region
Bowel sounds are sluggish
I/O : 1500/1100ml
GRBS: 112 mg/dl given (4units of HAI and 4 units of NPH)
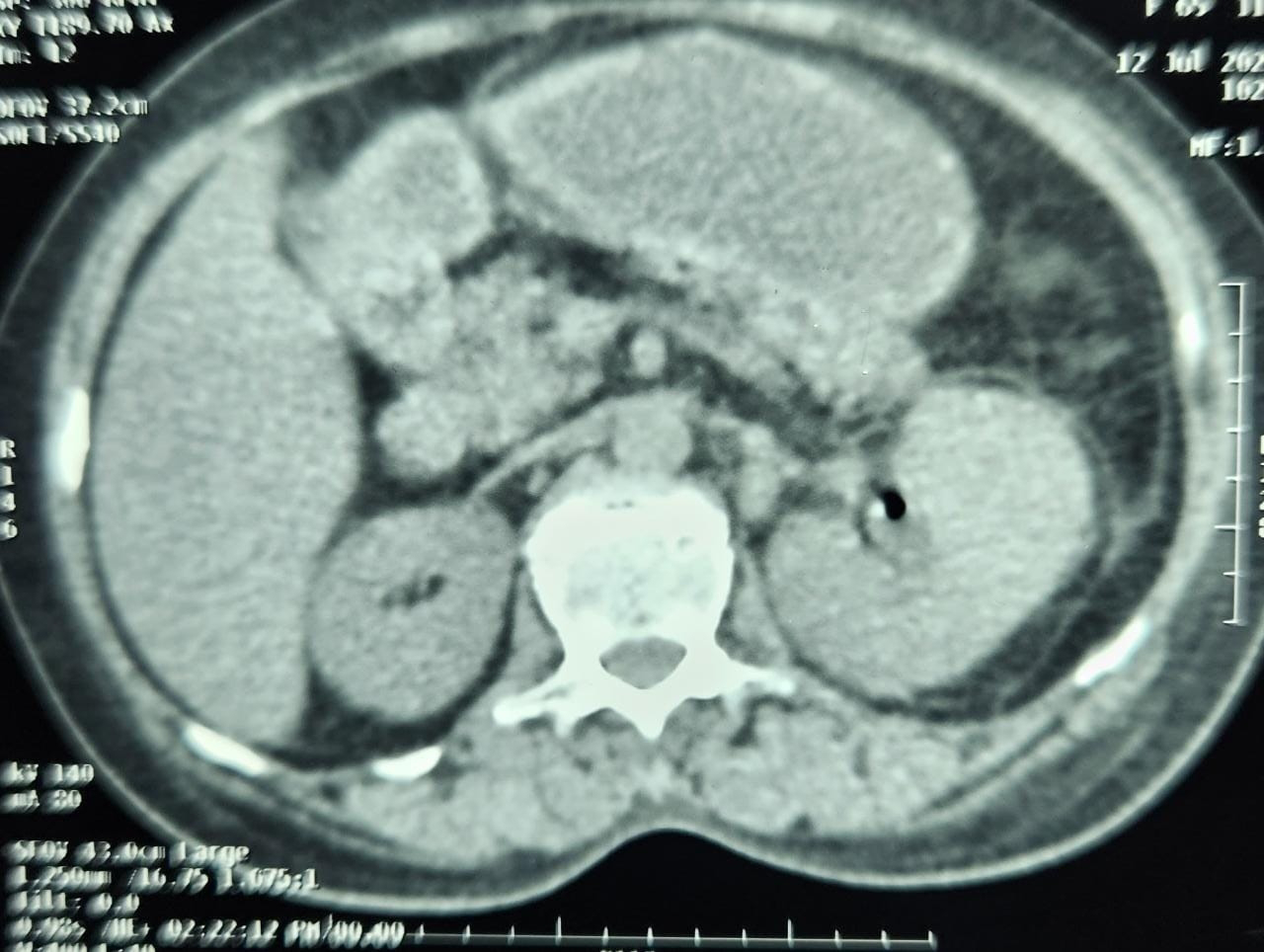
A: Left acute pyelonephritis
With AKI(resolved) secondary to left proximal ureteric calculus(?17mm) with type 2 DM and HTN since 25 yrs with anemia
S/p : cystoscope and guide wire placement (pod 2)
S/P: DJ STENTING WAS DONE UNDER LA YESTERDAY
1)IV fluids
Ns,RL@50ml/hr
2)Inj.Piptaz 2.25gm IV/TID
3)Inj.Tramadol 1amp in 100 ml NS IV/BD
4)Tab Cinod 10mg po/BD
5) Tab. Nicardia 10 mg po/sos
6) Tab Dolo 650 mg Po/TID
6)Strict I/o charting
7) GRBS 7. Profile
8)Inj. HAI S/C21/7/23
Pain subsided
No fever spikes, vomitings
O: patient is c/c/c
Afebrile
PR: 84 bpm
Bp: 170/80 mmhg
RR: 18/min
Spo2 - 98% on RA
CVS: S1 S2 heard
No murmurs
Rs: BAE +
NVBS
CNS: NAD
P/A : No tenderness
Input : 2400ml
Output:2200ml
GRBS: 124 mg/dl (6units of HAI and 4 units of NPH given)
A: Left acute pyelonephritis
With AKI(resolved) secondary to left proximal ureteric calculus(?17mm) with type 2 DM and HTN since 25 yrs with anemia
S/p : Cystoscopy and Guide wire placement under LA(pod 3)
S/P: DJ STENTING WAS DONE UNDER LA (Pod 3)
P:
1)Plenty of oral fluids
2)Inj.Piptaz 2.25gm IV/TID
3)Inj.Tramadol SOS
4)Tab Cinod 10mg po/BD
5) Tab. Nicardia 20 mg PO/QID
6)SYP.Alkastone B6 15ml in 1/2glass of water PO/BD
7)Strict I/o charting
8) GRBS 7. Profile
9)Inj. HAI S/C TID
10)Inj. NPH S/C BD























No comments:
Post a Comment